
What is Fascia and is it Important for Massage?

If you’ve spent even just five minutes searching for pain treatments, then you’ve most likely ran across a dozen articles preaching the gospel of fascial therapy. It’s the current it thing in alternative medicine - heck, it’s plastered all over this very website. With that, you might be asking yourself, “wait, what exactly is fascia? Is mine damaged? Is that why I’ve been in so much pain?” Well I’m here to help you on that journey. I’m a fascia focused massage therapist who doesn’t actually believe fascia is the structural cause for a majority of our daily aches and pains. That doesn’t mean that it’s not fascinating or that it’s totally irrelevant for manual therapy though! In this post, we’ll explore how treating fascia is ripe with opportunities for new ways of relating with ourselves and how we move through life. First though let’s clarify what this tissue is…and isn’t.
So…what is it?
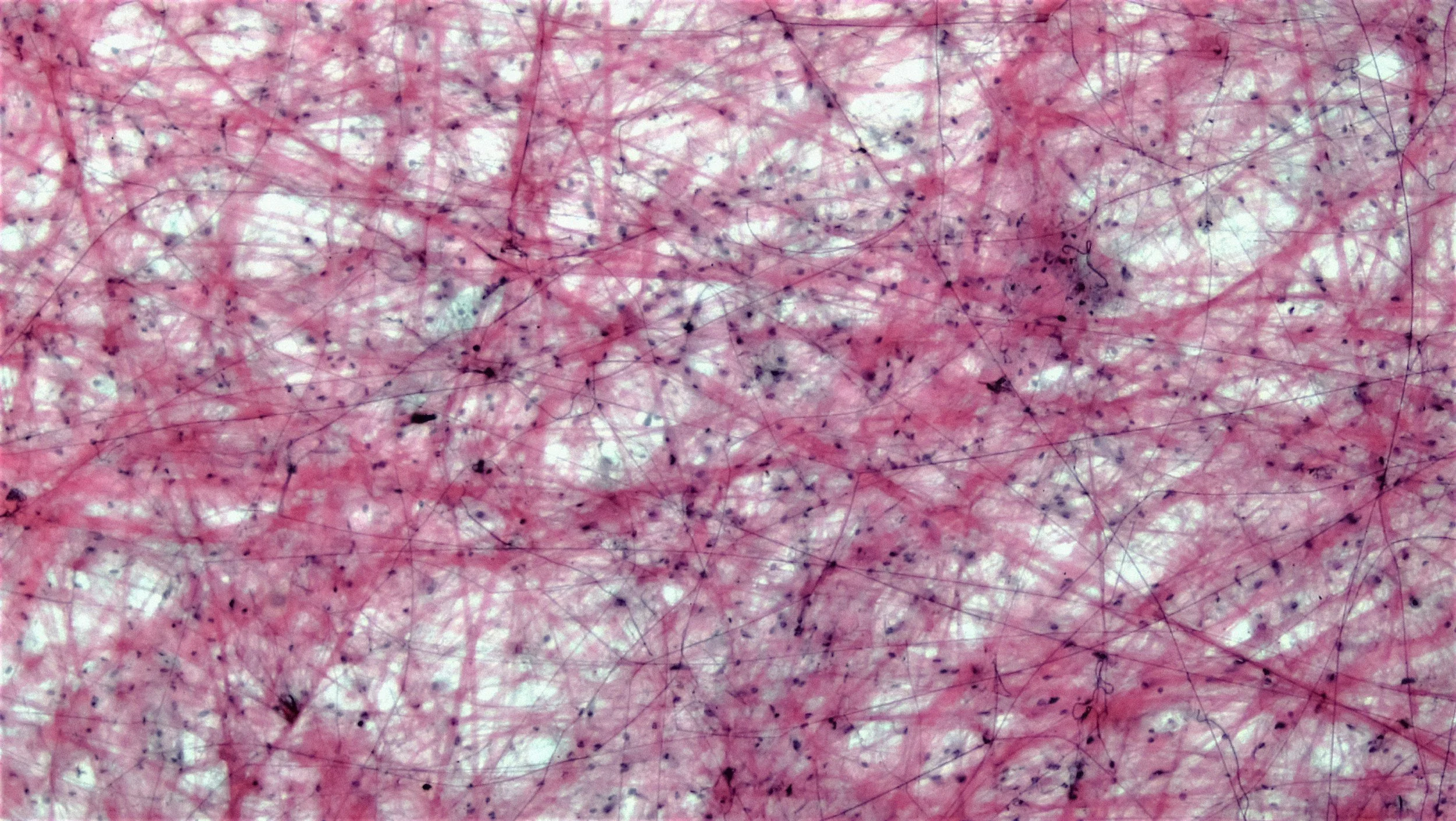
Fascia is one of the body's main forms of connective tissue. It's a cohesive three dimensional webbing primarily made of collagen that spans from the top of your head all the way down to your littlest toe. Not only does it line the underside of your skin, it also weaves around and through each of your muscles, bones, joints, nerves, and blood vessels as one inter-connected whole. It can be thin in some places and incredibly thick in others depending on how that part of the body gets used. It’s essentially the tissue that ensures each individual piece of the body stays connected and working together. It’s often thought of as a sort of “packing material” which provides structural support to give our body its unique shape. At the same time, it’s also responsible for lubricating the muscles so they can glide across each other, allowing for fluid movement. That’s because unlike most tissues in the body, fascia is both fibrous and fluid — it's saturated with water and gel-like substances that keep its many layers from tugging or dragging on each other. If you were to look at it up close, it resembles a shimmering, silvery white film — delicate and translucent in some places, thick and rope-like in others, woven together like an intricate lacework. If you’ve ever eaten a good steak (if that’s your thing) then you’ve undoubtedly found yourself chewing on the white gristle that runs throughout the meat - that’s the fascia.
There are technically four distinct layers to the fascia; superficial, deep, visceral, and microscopic — though it's really one intricate, interconnected whole. It can still be useful to break these down for ease of understanding.
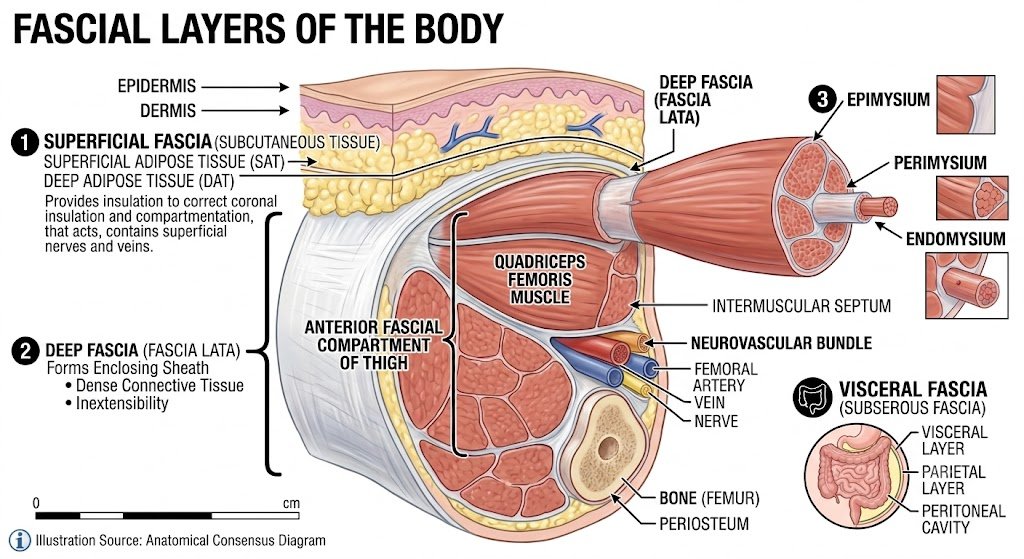
Superficial Fascia - This is the outermost layer underneath the skin. It’s there to store fat and water which serves as an insulation and passageway for nerves and blood vessels.
Deep Fascia - This is a more dense form of fascia that wraps around each of our muscles, bones, nerves, and blood vessels. We can think of them like sheaths that help support each of these elements.
Visceral Fascia - This fascia is wrapped around our organs and helps them keep them suspended within our body, providing stability and protection.
Microscopic Fascia - On the smallest level, this fascia wraps around individual muscle fibers, bundles of muscle fibers, and entire muscles themselves which grants muscles their ability to glide and move smoothly.
Beyond structural support, fascia also has the interesting role of helping us move through space. It does this by transmitting the forces from the mechanical tension generated by our muscles into our bones. This propels our bodies through the environment while simultaneously keeping us upright against the steady pull of gravity. It also has elastic qualities which stretch, twist, bend, and ultimately snap back, creating a spring mechanism which reduces muscle energy, making it easier for continued movement. To help with this process, fascia is also one of the most densely innervated tissues in the body. In fact, there are some regions of fascia that are nine times more innervated than muscle tissue. This is personally the part that starts to perk my ears up as a neurologically focused massage therapist. That’s nine times the amount of opportunity for novel sensation and creativity within a massage session!
The main receptors that are responsible for helping with the monumental task of moving our bodies are called mechanoreceptors. These are specialized receptors that are used for proprioception and tactile sensation. Proprioception is the body’s ability to automatically sense its own position, movement, and orientation in space without relying on vision. Without proprioception, it would be incredibly challenging to do anything physical with our bodies, we’d have no sense of where we are in relation to the things around us. Proprioception is what enables us to type on keyboards, itch our nose, walk on uneven terrain, or ride a bike - it’s essentially what we’re referring to when we talk about ‘muscle memory’. There’s an automatic quality to it, meaning that we don’t have to think about doing it, our body handles it under our conscious attention. This is just one example of the kind of sensory cells that are present in fascia though.
The other and most abundant kind of sensory cell present in fascia is what is known as a free nerve ending. These are the most common and unspecialized sensory receptors in the entire body. Their primary role is to detect pain, temperature, itch, and other forms of crude touch. The key suspects for our discussion of pain and therapy are nociceptors and chemoreceptors. If you aren’t a big science nerd like myself or haven’t explored any other articles in this blog, these cells serve as the body’s primary alarm system if there’s harm or even just the potential for harm. They detect things like intense mechanical deformation of the tissue, extreme temperature changes, and environmental irritants. When any of those conditions are present, they shoot off a signal to the brain in a process called nociception. These aren’t pain signals per-se as they don’t in and of themselves contain pain. Instead, the brain will take this nociception and form an opinion of sorts, combining it with other variables in the environment, our history, mental wellbeing, general health, and many more factors. If there’s enough of a case to indicate harm could have taken place, then it will create pain. All of this begins with nociceptors, of which many belong in the fascia! (Check this blog below for more information on that)
The last piece of the neurological puzzle come in the form of sympathetic efferent fibers which are directly responsible for maintaining our sympathetic tone. In other words, they serve as the bridge between the emotional states of our mind and the somatic experience of them in our body. When we’re feeling stressed, the brain will send signals along these nerves to activate the muscles to prime them for potential action. This feels like tightness to us. It’s not that the muscle itself is tight, but rather that the efferent fibers are receiving signals from the brain which feel like tightness. On the flip side, when we’re feeling relaxed, the brain tells these fibers that there’s nothing to worry about and they will calm, which we generally associate with the felt sense of being at rest. They’re also responsible for that sinking in your gut when you receive bad news, the tightness in your chest when you’re angry, or the nausea you might have when you’re grieving. I have a whole article detailing this over here: https://www.bkbodyworks.net/blog-1/why-safety-is-important-for-your-nervous-system-and-how-massage-can-help).

In summary, fascia is the connective web that binds all of our individual elements into one cohesive whole. It helps support our structure, move through the environment, and sense both our inner and outer worlds. Without it, we’d likely turn into piles of goo. Naturally this has led researchers into looking at the therapeutic effects of manipulating fascia, of which there is a long history of folks who’ve done so - but have they really had any solid results? Well, it’s a little more complicated than a majority of manual and physio therapists would like to admit. Most of the claims that are made in the fascial medicine communities revolve around the prospect of manipulating the tissue to enact some sort of physical change in it. This could be ‘making it looser’, 'hydrating it’, ‘busting up adhesions’, etc etc. While the practices that emerged from this understanding do provide relief for millions of people across the globe, the mechanisms behind them have been thoroughly debunked in a very real way. The more modern understanding points us in the direction of the neurological implications of working with the fascia. I want to take a moment to go through some of the big claims made by therapists over the years and explain where they went wrong. I then want to make the case for why working with the fascia is still important despite all of that and share some of the latest perspectives. Let’s get started!
Components of Fascia and their Respective Therapies
In order to better understand the mechanisms of fascial therapy, we’re going to need to look at the building blocks of the tissue itself. These are where many therapies are claiming to affect change so it’s important to understand their intrinsic qualities to explain what’s possible (or not) in working with them.
To start, let’s get a very strong microscope to look inside of the fascia on the cellular level. If we were to do that, what we would find is a goopy substance filled with little particles of all different shapes and sizes. This gel like “goop” is called the ground substance, it’s a mixture of water and hyaluronic acid. This is a slippery, viscous fluid that lubricates the layers of fascia, which allows them to glide smoothly over one another as you move. The quality of this substance varies depending on where you look in the body, it’s more liquid in some places, and more fibrous in others. The ground substance in the ligaments of your elbow is going to be quite different than the ground substance in the belly of your bicep. Yet, they are still considered one continuous whole, an inner ocean if you will. Contained within that ground substance is a combination of different fibers, proteins, and specialized sensory cells, all of which come together to create what’s known as an extracellular matrix (ECM).
In terms of the important players that are floating in the ECM, we have two major ones which determine the physical qualities of the tissue. The first one is collagen, which is the most abundant protein in your body. This is the component of our fascia that glues tissues together, provides structural support, and elasticity to our skin, giving us that smooth look of young skin. As we age, our collagen production naturally begins to decline, leaving us with wrinkles and diminished strength. The second physically defining component floating in the ECM is the elastin. This is a highly elastic protein which acts like a biological rubber band, allowing tissues to stretch and then recoil back to their original shape. Without elastin, important organs like our heart and lungs wouldn’t be able to function properly. It also provides the same benefits to our muscles, helping reduce the energy cost of movement.
Outside of the essential proteins that establish our structure, there are tons of different specialized cells within the ECM as well. There are the classic mechanoreceptors (classic in the sense that every bodyworker learns about them), such as the Ruffini Receptors, Pacini Corpuscles, Golgi Organs, and the Interstitial Receptors. Each of these detect different forms of sensory input, whether it’s vibration, touch, pressure, stretch, and muscle tension. This enables us to sense into our environments, feel our surroundings, and balance against the force of gravity. Beyond the mechanoreceptors and sometimes included in them are also the Free Nerve Endings that I mentioned above. These are all very interesting in their own right but what I want to focus on is the ground substance and the two physically defining proteins. These are the main components that many fascial therapists are claiming to affect change on, so let’s look at those claims and whether they hold any water.
Ground Substance and ‘Lubricating the Tissue’
One of the primary claims made by fascial therapists is that the ground substance of underutilized fascia will become dry and sticky. This is said to cause the fascial layers to not glide as efficiently, tug, and ultimately cause restriction and pain. This is why movement and massage is encouraged so often, the mechanical forces are said to lubricate the fascial layers and restore functional fascia. The principle behind this is that of thixotropy which is a quality within certain tissues to move from gel (sticky, thick,) to sol (liquid, viscous) and vice versa. While the thixotropic effect is a known quality in many parts of the body including our blood, mucus, synovial fluid, and yes, our fascia, it hasn’t been shown to be a contributor to the sensation of pain or even a reduced range of motion. If you want to look for yourself, here’s an excellent study done by one of the world’s leading fascial researchers, Dr. Robert Shleip: (https://www.sciencedirect.com/science/article/abs/pii/S1360859202000670).
Even if there were some compelling data to work with - the issue with this is that thixotropy is quite minor, slow, and most important, temporary. It tends to revert back to its baseline after just a few minutes of the mechanical pressure being removed. The alternative hypothesis is that the heat of the contact is what does the “softening” but if that were the case then a hot summer day would likely lead to a mass medical event.
To strengthen the argument, even one of the grandmothers of fascial medicine, maybe the most influential figure in all of fascial therapy and the progenitor of the thixotropy hypothesis, Dr. Ida Rolf, eventually cast some serious doubts onto the idea later in her life. She’s quoted as saying “… under your hands you feel the change. Now this is going to call for some smart researching sometime. And who’s going to do this I don’t know. I hope somebody is going to come out of the blue who is going to be peculiarly well-fitted for this kind of a job. And I haven’t the foggiest idea what it means. Possibly it means a general change in pH of the tissue locally. Possibly it means, this is the simplest way to express it, the greater energy that goes in there and makes the sol, the gel a sol. Possibly this is what it means. This is what I’ve taught that it means. But this is a nonsense teaching really! What does it make into ‘sol’? Does it make the wall of the blood vessel sol? This is absurd!”
So if the founder of this idea wasn’t totally convinced that it was a plausible explanation, then I’m personally not going to give it too much stock. Even if we were able to successfully create change in the fluid dynamics of ground substance in any lasting way, there’s also been no connection in the research to indicate that it would actually help us hurt less.

Sand is a great example of another thixotropic substance.
Collagen and ‘Breaking Up Adhesions’
Adhesions, restrictions, tightness, shortening, knots: how many times have you heard these phrases from your massage therapist or otherwise? It’s what we were taught in school so it makes sense that would be the main diagnostic model that we have for our work. The issue is, there’s very little to no evidence that many of these things physically exist, and those that do, have weak evidence connecting them to pain. Let’s take a closer look at the main ones regarding fascia:

Adhesions and Knots:
This description carries the most weight out of the above listed issues people face regarding their fascia. Manual therapists absolutely love to point out how an adhesion is causing your pain and that it needs to be broken up. While adhesions certainly do exist, especially in a tissue that has a history of injury (scar tissue is an adhesion), smaller less obvious ones are not reliably able to be detected through touch. (Source: https://pubmed.ncbi.nlm.nih.gov/19158550/) Even if they were, there’s been no causal evidence showing that they have any relationship to pain. This doesn’t negate the fact that the experience of a “knot” exists though. What’s known as a ‘Myofascial Trigger Point’ is a very well documented phenomenon that I’m sure anyone reading this has had the experience of. What it is though is not quite as clear, with many different theories emphasizing different possibilities. The most accurate answer we have right now is that they’re neurological in nature or an issue with the individual muscle fiber cells. This is quite a different explanation than the bundled up muscle tissue that we imagine. I’ll definitely be writing a whole article on this subject in the near future.
Restrictions, Shortening, Tightness:
Fascia can come in many levels of density, there’s thinner fascia at the surface and denser fascia at more critical junctures (like our low-back or surrounding joints). While there is a universal map of where the densities are thicker across people - there’s going to be some unique differences between people, since every body is different. I may have denser fascia in one part that’s loose for you, yet I may still be more flexible in that region. That’s because flexibility and Range of Motion (ROM) have much more to do with the nervous system than our physical structure, which explains why two people with identical tissue density can have dramatically different levels of flexibility. So I think it’s useful to reframe this notion of restriction as a reduced sensory awareness, heightened threat perception, and activated nervous system tone.
Even if the evidence were pointing to our pain being caused by a physical adhesion or restriction in the fascia, that is to say a buildup of collagen from overuse, misuse, or improper healing - collagen is…very very strong. In fact, its closest comparison would be to that of Kevlar (the material used for bulletproof vests). The notion that we would be able to break apart or bust up this adhesion using mechanical forces from our body would be like rubbing a hole in a leather belt. Even if we could do that, the amount of pain it would cause would be infinitely worse than the original issue that was bringing the client to bodywork. Keep this in mind the next time a practitioner of any profession recommends that you undergo a rigorous scraping session. Unless you like the sensation of having your skin flayed off your body. (Yes this is a real treatment and no it does not do what it’s marketed as doing).
Elastin and ‘Increasing Flexibility’
One of the other popular theories when it comes to fascial medicine is that by introducing slow, medium to high pressure holds on the tissue, it will deform and take on a more ideal and flexible state. This is claimed to be a result of stretching out the elastin fibers and allowing them to recoil back to a new and more elongated baseline. This is the primary explanation for why stretching and yoga are so beneficial for us as well - it makes our tissue more elastic. Shockingly though, even this hypothesis is being challenged pretty competently in recent years. With evidence showing that our range of motion and overall flexibility is determined less by the extensibility of our muscles and more from our tolerance to the intensity of stretch sensations. (Sources: https://pubmed.ncbi.nlm.nih.gov/16515422/ and https://pubmed.ncbi.nlm.nih.gov/24947023/). There may be some therapeutic implications for increasing our tolerance to uncomfortable sensations, but that’s a different sales pitch than making our muscles more physically flexible.
The distinction there is that this process of increasing our tolerance to stretch sensations takes a long time. Much more than what’s available to clients in a weekly 60 minute session. In that study alone, they had to set up a four week experiment which required participants to stretch for 20 minutes every single day. Even in that instance, there were no noticeable increases in the angles their muscles were able to stretch to, despite being able to withstand greater degrees of torque. A more realistic perspective would need to take a long view in terms of years of daily practice and effort. If it took any less then we would be in some serious trouble whenever we went on a long car ride, as our body would start to deform from sitting in the seat. In order for us to genuinely become more pliable in a real physical way, we would have to reshape our collagen over long periods of time, which we already discussed as being quite difficult.
This is good news though! For if it were any different, then an unskilled massage therapist could easily cause us harm as they unknowingly reshaped our fascial web in a way that impaired us rather than helped. What’s doubly good about this news is that - it probably doesn’t matter for our experience of pain how stretchy our fascia is. What a relief! Now you might be saying to yourself…”man, it really sounds like this fascial therapist doesn’t believe in working with fascia”. On the contrary, I find it to be endlessly fascinating. There are a ton of therapeutic implications found in working with this tissue beyond the mechanical wear and tear model that a majority of therapists find themselves stuck in. Let’s go back for a moment to look at the neurological qualities of fascia
Why I Still Emphasize Fascia in my Treatments
As noted above, fascia is often considered the organ of embodiment. It’s one of the main tissues responsible for our sense of proprioception; that being our bodies innate sense of its movement, position, and balance in space. This is a core aspect of what it means to feel in our bodies, which is an increasingly rare quality for people to have. As technology has advanced and our world has gotten more chaotic, we tend to spend more and more time in our phones or strategizing in our heads how to navigate the complexity. We’re essentially living as if we’re floating heads carrying around the dead weight of our body - only sensing into it when something goes wrong with it. This disconnect from the body keeps us from being able to listen to the messages that it’s sending until they get so loud that it demands that we respond - usually through pain or discomfort. The goal then in working with fascia is to soak it with our awareness and “wake it back up”. In more technical terms, the fascially focused therapy should emphasize the activation of the multitude of different sensory nerve endings that exist within the fascia. Without consistent sensory stimulation, whether it be movement or manual therapy, the neural pathways connecting these cells to the brain weaken and we lose their sensitivity - dulling our body’s ability to hear and be heard. It’s the classic ‘use it or lose it’ principle.
So what happens when we don’t have a strong sense of our bodies? Well for starters, when we’re in pain, it REALLY hurts, because there’s no broader context for the pain to exist within. It’s just our thoughts, and the pain, and our thoughts, and our pain. What if instead of those two elements bouncing off from each other, we also had a lucid awareness of the ease within another part of our experience? That contrasting ease can serve as a resource for us in relating differently to our pain, and might even grant us a window of opportunity to move and live our lives just a little more normally. Another element of being in touch with our bodies is that there are less surprises in the nervous system when we’re performing an action that we may not be used to. A “dull” body sense is more likely to respond to external stimulus with alarm, which in body-speak, is pain. (remember, pain is about injury prediction rather than a 1:1 report of what’s actually happening in the tissues. It occurs as a means to protect us before we are harmed). On the contrary, a body that is primed for a wide range of sensory stimulation has more information at its disposal to interpret signals as within the acceptable and expected range of possibilities. This means that it won’t ring the pain alarm when lifting that heavy box because it’s awake and pliable. Just think, if you were helping a friend move, wouldn’t you want to have had a cup of coffee and breakfast first? It would suck to hop right out bed and into the moving van. The body is the same way.
The reason that I emphasize fascia in my therapy is because of this: the techniques that emphasize fascia incorporate more of the sensory system than most other manual therapy modalities. The long, slow, stretching strokes activate different sensory cells than a faster well-oiled stroke. There’s a degree of dimensionality to this approach that you won’t find in deep tissue, regular Swedish, or medical massage. The goal isn’t to change the physical structure of the fascia, it’s to speak to it in as many different languages as possible. Ideally this therapy would be coupled with a robust kinesthetic diet of unique movements to ensure a wide range of novel inputs. For some of us though, it’s challenging and often painful to begin a new movement practice - fascial therapy in this sense can serve as a wonderful foundation to begin experiencing our body in different contexts. The more ways we move and sense, the wider our capacity to attend to the lives that we’re living, including our pain.

Another element that I appreciate about the slow stretching motions is that it allows the brain a chance to more fully connect with the incoming sensation. In my experience, many massage therapists are over-lubricating and moving much too quickly. This can feel great in its own right but misses out on a lot of opportunities for the brain to form a deeper relationship with the contact that’s being provided. When we slow our work down, it creates a space for the brain to make more connections with what’s happening, which allows it to have a more meaningful and profound experience. This quality of ‘meaningfulness’ isn’t necessarily a scientific term but it is something that clients have reported to me time and time again. What does it mean though? I think this will vary from client to client but my sense is that it’s an expression of the touch having mattered to their experience of pain. It’s a way of simultaneously letting the nervous system know, ‘I see you and this hurt’, and also ‘you’re okay’. This subtle unspoken communication conveys a sense of safety that has a real effect on our autonomic nervous system, our emotional body, and even the way we cognize our pain.
The slower more intentional pacing also provide more opportunities for variation within each individual stroke. We can start and end at the same places but the journey of how we get from A to B can be wildly different. One pass could incorporate some gentle rocking while another has alterations of pressure which create a pulsing effect. We can play with different applications of pressure, directions we take the tissue in, or even which part of the hand we’re using to apply the pressure. This is much more interesting to the nervous system than applying the same static pressure at the same static pace that many modalities rely on.
So to summarize, fascia is a sensory organ. Its evolved to sense into the world around us and to relay information to our brain about whether or not we’re in a safe environment. Techniques that target the fascia (which if we’re being nitpicky is every single massage technique in existence) have a unique opportunity to maximize the amount of calming signals going to the brain. The slower pace of the strokes creates an opportunity to dialogue with the body in hopes that we can remind it how to slow down.
Actual Fascia Pathologies
So with everything I just mentioned above, I do want to be clear - there are certainly some fascial pathologies that exist within the structure of the organ. Their relevance to the world of manual therapy is overstated as the symptoms of these pathologies are quite intense and often unavailable to be worked with directly. Massage can be effective in helping the person with these ailments cope and relate with their experience differently but there haven’t been any known fixes - manual or otherwise. Below are some of the more common ones (though still very uncommon in the broader picture).

Dupuytren’s Contracture
Just as soon as I’ve been questioning the mechanical restriction model, here comes a legitimate disease of the hand whose main symptom is contracture. Thus is the practice of medicine I suppose. In this condition, the fascia of the hand beneath the palm starts to thicken and shorten, which eventually will begin curling the fingers inward. It’s often painless but will begin to interfere with daily tasks if left untreated. We don’t really know what causes it at the moment but it seems linked to abnormal cell activity that creates excess amounts of collagen in the hands. Men above the age of 50 are the most affected.
Seeing this is useful because it highlights what a real contracture in the fascia looks like. So unless you’re recognizing something of this quality, rest assured you probably don’t have a physically tightening fascia.
Ehlers-Danlos Syndromes
This one can be a real doozy. EDS is a group of hereditary connective tissue disorders that affect the collagen production in our fascia. As we discussed above, collagen is what provides the structure and elasticity to our skin, joints, and other tissues. With this disease, the connective tissue in the body becomes fragile and less resilient. The symptoms vary from person to person but they commonly include joint hypermobility, unexplained chronic pain, unusually soft skin, and a slower healing time for wounds. It has been known to affect the organs in certain circumstances causing fatigue, digestive issues, and heart rate irregularities.
Massage in this case needs to be approached with care and kept within an appropriate pressure range. Work that’s too intense can cause bruising and other sustained injuries deeper in the tissues. Very important to communicate with your therapist if you have this so they know how to work with you!
Myofascial Pain Syndrome
MPS is a condition in which numerous painful trigger points appear throughout a region of the body. It can be acute or chronic depending on a number of different factors that aren’t totally clear to us yet. Pain is known to be both localized and refer outward to other parts of the body that don’t appear to be related in any capacity. It’s likely responsible for anywhere between 30%-90% of chronic musculoskeletal pain (big window, I know) and tends to affect those between 27-50. Despite its widespread prevalence, we’re not totally sure what exactly causes MPS….or what cures it. It’s generally recommended to combine a number of different modalities depending on the unique circumstances of the patient’s life. It’s not uncommon to be recommended stretching routines, manual therapies, dietary changes, talk therapy, and posture alterations.
The lack of clear understanding on this pathology speaks volumes of just how understudied musculoskeletal pain is in the world of medicine. We’re making some great advancements in the past couple of decades but it’s still considered a fledgling field of study in the broad scope of science. That’s both exciting and frustrating!

Plantar Fasciitis
Plantar Fasciitis is probably one of the most well known conditions on this little list here. Luckily it’s also one of the most well understood and treatable. PF occurs when the thick band of fascia on the heel of the foot becomes irritated and inflamed. This section of fascia called the ‘Plantar Fascia’ helps connect the bones of your foot and forms the bottom arch in your foot. It can be irritated for a number of different reasons including: spending too much time on your feet, not having proper footwear, or playing too many sports. When this happens, we can experience heel pain, stiffness, swelling, and it’s generally very painful to walk. Symptoms do tend to feel better rather quickly when we begin to start treating it.
Treatment can include icing, self or professional massage, getting new footwear, and finding ways to get off our feet for a little bit. What I’ve found to be a good practice is to buy a tennis ball and put your weight onto it, applying pressure and rolling it around the entire bottom of the foot. Doing this multiple times a day tends to “loosen” it up a considerable amount. Doing this when we don’t have pain also helps us make sure that it doesn’t develop!
In Conclusion
Fascia is a fascinating tissue. It’s rise in alternative medicine is largely understandable given its prevalence in the body and its relatively small pool of well structured studies. Much of the research is coming up fairly inconclusive on the overall effectiveness of classic myofascial focused therapies but anecdotally - the buzz is there. Millions of people all across the world are swearing up and down that its helped them overcome some incredibly tricky pain situations. I’ve even experienced it myself as a practicing massage therapist over the past six years. Despite my skepticism on many of the claims made about fascial therapy, the intention with this article is not to dissuade anyone from seeking out these treatments if they feel called to them. Rather, I think its important that we have a clear understanding of what we do (or don’t) know about the tissue itself - of which there is a growing amount. The proper framing can change the way we view treatments, and may even change the outcomes of our sessions. Having a leveled, evidence constructed perspective of what’s possible with any form of physical or manual therapy equips us with the tools to make informed decisions about our care. I’m sure that as the years roll on, new interesting evidence will emerge that may even rattle the pillars of this article. In those instances, its important that we as healthcare professionals adapt and change our models to meet what the current science is showing. In the meantime though, what we have is a collection of tools and techniques which provide incredibly unique experiences for our clients. They’re experimental in nature and should be communicated as such - but at the same time, so is most of the physical therapy profession, chiropractic work, and the rest of manual therapy. The truth is, helping people in pain is never a one size fits all journey. Each person is going to respond differently to different things. It’s our job as practitioners to simply be honest in our assessment, transparent in our understanding, and flexible in our treatments.
To cap this whole thing off, here’s a conversation that I recorded some years ago with one of the world’s leading fascial movement practitioners, Thomas Myers. He’s the founder of the Anatomy Trains program which is one of the biggest fascial therapy methodologies in the world. In it, we discuss the importance of moving beyond the physical explanations of fascial therapy and why we should bring our attention to the nervous system. Enjoy!
References
‘Can fascia’s characteristics be influenced by manual therapy?’ - Serge Gracovetsky
https://pubmed.ncbi.nlm.nih.gov/27814871/
‘Fascial plasticity - a new neurobiological explanation’ - Robert Schleip
https://www.sciencedirect.com/science/article/abs/pii/S1360859202000670
‘Do manual and instrument-assisted myofascial release techniques truly change tissue stiffness? A systematic review an meta-analysis of randomized controlled trials with GRADE assessment’ - Kunz and co
https://www.sciencedirect.com/science/article/abs/pii/S136085922600166X?__cf_chl_f_tk=_OyOZzyxNQhU22LhCjKSQCuw5j36yWcGwhybaB4586k-1783368021-1.0.1.1-HHSURcf.8UaLQox7IWoAAkL.NYKfll.0DsRptAeKKCE
‘Does Fascia Matter?’ - Paul Ingraham
https://www.painscience.com/articles/does-fascia-matter.php